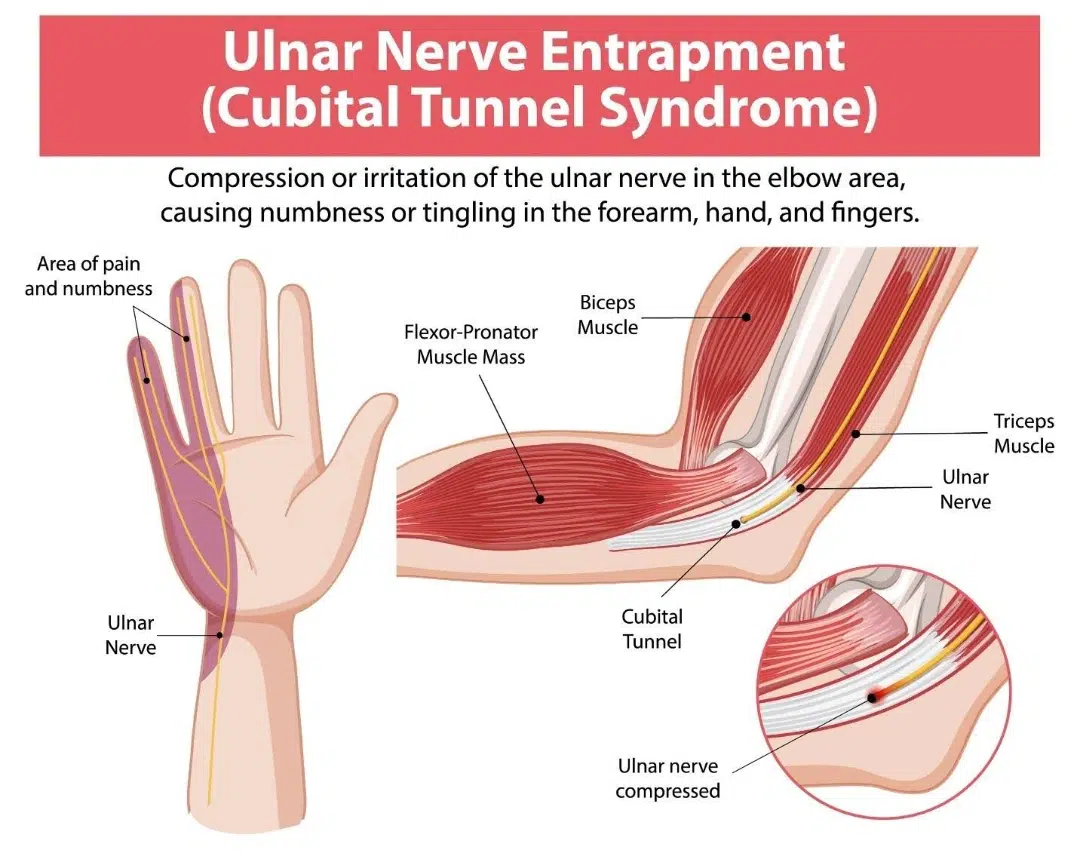
Cubital Tunnel Syndrome is a condition caused by compression or irritation of the ulnar nerve as it passes through the cubital tunnel, which is a narrow passage located on the inner side of the elbow.
The ulnar nerve, commonly referred to as the “funny bone nerve,” plays a crucial role in controlling muscle movement, and sensation in the forearm, hand, and fingers.
Individuals with cubital tunnel syndrome may experience numbness, tingling, weakness or pain in the ring and little fingers, especially when bending the elbow for prolonged periods. Delaying treatment will result in muscle weakness, and loss of hand function, affecting daily activities such as gripping objects or typing.
The ulnar nerve originates from the cervical spine, and travels down the arm, passing through the cubital tunnel at the elbow before extending into the hand. Unlike other nerves, the ulnar nerve lacks significant protection from muscles or soft tissues as it runs through this narrow tunnel. This makes it particularly vulnerable to compression or irritation, especially when the elbow remains bent for extended periods.
The ulnar nerve is responsible for sensory, and motor functions in the forearm and hand, including:
Controlling fine motor movements in the hand.
Enabling grip strength and finger coordination.
Providing sensation to the ring and little fingers.
What causes Cubital Tunnel Syndrome?
Several factors contribute to the development of cubital tunnel syndrome, including:
Anatomical variations – some individuals have naturally narrower cubital tunnels, making them more prone to developing this condition.
Arthritis or bone spurs– conditions like osteoarthritis can lead to joint changes that exert pressure on the ulnar nerve.
Prolonged pressure on the elbow– leaning on the elbow for extended periods can compress the nerve within the cubital tunnel.
Previous elbow injury– fractures, dislocations or trauma to the elbow can cause structural changes that narrow the cubital tunnel, increasing nerve compression.
Repetitive elbow flexion – frequent bending of the elbow, such as during phone use, typing or resting the arm on hard surfaces, can increase pressure on the ulnar nerve.
Swelling or fluid retention– inflammation or fluid buildup around the elbow can contribute to nerve compression.
A tingling sensation or numbness in the ring, and little finger is one of the most common symptoms of cubital tunnel syndrome.
What are the symptoms of Cubital Tunnel Syndrome?
Cubital tunnel syndrome is often presented with:
Hand weakness or difficulty moving fingers– struggling to control or move the fingers properly, especially when they feel numb.
Inner elbow pain– discomfort or aching along the inside of the elbow, sometimes radiating down the forearm.
Intermittent numbness and tingling – a sensation of "pins and needles" in the ring, and little fingers, which may come and go.
Tingling sensations that fluctuate– episodes of tingling in the fingers and hand, particularly after prolonged elbow bending.
Additionally, the most obvious sign of cubital tunnel syndrome is numbness or inner elbow pain that typically worsens when the elbow remains bent for extended periods, such as when:
Driving
Holding a phone
Sleeping
Activities that involve excessive elbow flexion, such as holding a phone, typing or sleeping with bent arms, can put pressure on the ulnar nerve.
Who is at risk of Cubital Tunnel Syndrome?
Although cubital tunnel syndrome is uncommon in Singapore, there are certain groups of individuals that are more susceptible to the condition. This includes:
Bone or joint conditions–arthritis, bone spurs or anatomical variations in the elbow joint can contribute to nerve compression.
Diabetes or nerve-related conditions– individuals with diabetes or other conditions affecting nerve health may be more susceptible to developing nerve compression syndromes.
Direct pressure on the elbow – leaning on the elbow for extended periods, such as resting it on a desk or armrest, can compress the ulnar nerve.
Frequent or prolonged elbow bending– activities that involve excessive elbow flexion, such as holding a phone, typing or sleeping with bent arms, can put pressure on the ulnar nerve.
Previous elbow injuries – fractures, dislocations or trauma to the elbow can lead to structural changes that make the ulnar nerve more vulnerable to compression.
Repetitive elbow movements– jobs or sports that require repeated bending and straightening of the elbow, such as weightlifting, baseball or carpentry, may increase the risk of irritation.
Is Cubital Tunnel Syndrome the same as Carpal Tunnel Syndrome?
Although cubital tunnel syndrome, and carpal tunnel syndrome are both nerve compression conditions that affect the hand, they involve different nerves, and present distinct symptoms.
Some of the key differences between the two conditions are:
Feature
Cubital Tunnel Syndrome
Carpal Tunnel Syndrome
What is it?
Compression of the ulnar nerve at the elbow.
Compression of the median nerve in the wrist.
Causes
Repetitive elbow bending, prolonged pressure on the elbow, previous injuries.
Repetitive hand or wrist movements, wrist injuries, and fluid retention.
Nerve affected
Ulnar nerve.
Median nerve.
Fingers affected
Ring and little fingers.
Thumb, index, middle, and part of the ring finger.
Symptoms worse when
Elbow is bent, such as when holding a phone or sleeping.
Wrist is bent, such as when typing or gripping objects.
How is Cubital Tunnel Syndrome diagnosed?
Cubital tunnel syndrome involves a combination of diagnostic measures, namely:
Initial Assessment
A comprehensive evaluation begins with an initial assessment to understand the patient’s condition, and identify potential risk factors. This includes:
Assessing medical history – our orthopaedic specialists will review the patient’s medical history, including past injuries, repetitive activities, underlying conditions, such as arthritis or diabetes, and occupational or lifestyle habits that may contribute to nerve compression.
Assessing symptoms – our orthopaedic specialist will ask about the nature, frequency, and severity of symptoms. This will include numbness, tingling, pain, and muscle weakness in the hand, and fingers.
Evaluating symptom patterns – our orthopaedic specialist will assess whether symptoms worsen during specific activities, such as prolonged elbow bending while using a phone or sleeping, to determine the extent of nerve involvement.
Physical Examination
Following an initial assessment, our orthopaedic specialist will conduct a thorough assessment to determine the severity of nerve compression, and identify the affected area. To confirm the diagnosis, our orthopaedic specialist will perform one or a combination of the following tests:
Tinel’s Sign Test – Tinel's sign test involves gentle tapping over the ulnar nerve at the elbow to check for tingling or an electric shock-like sensation in the ring, and little fingers. If present, it will indicate nerve irritation.
Elbow Flexion Test – an elbow flexion test involves asking the patients to bend their elbow, and hold the position for a period of time to see if symptoms such as numbness, tingling or pain develop. The test will enable our orthopaedic specialist to assess nerve compression.
Grip and Pinch Strength Tests – grip, and pinch strength involves evaluating a patient's ability to grip objects, and pinch between the thumb, and fingers, as muscle weakness can be a sign of advanced nerve compression.
Sensation Testing – sensation testing involves light touch or pinprick tests may be performed to check for reduced sensation or numbness in the affected fingers.
Imaging Tests
In the event further evaluation is needed, imaging tests may be recommended to confirm the diagnosis, and rule out other conditions affecting the elbow or nerves.
Ultrasound – an ultrasound provides a real-time view of the ulnar nerve, allowing the specialist to assess nerve compression, swelling or subluxation, which refers to nerve movement that is out of place.
Magnetic Resonance Imaging (MRI) – MRI scans offer detailed visualisation of the soft tissues, including the ulnar nerve, muscles, and surrounding structures. This is useful for detecting nerve inflammation or structural abnormalities.
X-rays – while X-rays do not show nerves, they may be used to rule out bone-related causes of nerve compression, such as fractures, bone spurs, or arthritis in the elbow joint.
Nerve Conduction Studies and Electromyography (EMG)
In some cases, electrical tests may be conducted to assess nerve function, and pinpoint the location of compression.
Nerve Conduction Studies (NCS) – NCS measures the speed, and strength of electrical signals traveling through the ulnar nerve, helping determine the severity of nerve compression.
Electromyography (EMG) – EMG evaluates muscle activity by detecting electrical signals in the muscles controlled by the ulnar nerve. It can identify muscle weakness or nerve damage associated with prolonged compression.
How is Cubital Tunnel Syndrome treated?
The treatment for cubital tunnel syndrome depends on the severity of symptoms. In mild to moderate cases, conservative approaches can relieve symptoms, while severe or persistent cases may require surgical intervention.
Conservative (Non-Surgical) Treatments
Activity modification– avoiding activities that keep the elbow bent for prolonged periods or that put direct pressure on the nerve. Using a headset instead of holding a phone, adjusting desk ergonomics, and avoiding leaning on the elbows can help alleviate the symptoms.
Bracing or splinting– wearing an elbow brace at night can prevent excessive bending during sleep, reducing pressure on the nerve.
Physical therapy– stretching, and nerve-gliding exercises may improve mobility, relieve tension on the ulnar nerve, and reduce symptoms. Additionally, strengthening exercises for the forearm, and hand muscles may also help in improving the condition.
Anti-inflammatory medication– non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen can help reduce pain, and swelling.
Cold or heat therapy– applying ice packs to reduce inflammation or using heat therapy to relax stiff muscles may provide symptom relief.
Injection Therapy
Corticosteroid injections – our orthopaedic specialist may administer corticosteroid injections to temporarily reduce inflammation, and relieve symptoms. However, these are generally used sparingly to avoid potential side effects on nerve health.
Surgical Treatments
Ulnar nerve decompression– this procedure releases pressure on the nerve by removing constrictive tissue or widening the cubital tunnel.
Ulnar nerve transposition– the surgeon moves the ulnar nerve from its original position behind the elbow to a location where it is less likely to be compressed.
Medial epicondylectomy– in cases where the bony prominence is contributing to nerve compression, a portion of the bone may be removed to create more space for the nerve.
Rehabilitation and Recovery
Post-surgical care– after surgery, the arm may be immobilised for a short period. This is then followed by a structured rehabilitation plan to help the arm regain its strength, and mobility.
Gradual return to activity– patients are also advised to avoid repetitive elbow movements initially. To facilitate recovery, patients will be required to follow a gradual return to daily activities.
Physical therapy– physical therapy is an essential part of recovery as rehabilitation exercises can help restore strength, flexibility, and nerve mobility.
After an orthopaedic confirms cubital tunnel syndrome, a treatment plan will be outlined to alleviate symptoms, and improve functionality.
Conclusion
Cubital tunnel syndrome can impact daily function and quality of life, particularly if it is left untreated. It is important to understand that seeking timely medical attention can help in preventing long-term nerve damage.
In fact, with appropriate treatment, most individuals can achieve significant symptom relief, and restore hand function. If you are experiencing persistent numbness, tingling or weakness in your hand, schedule a consultation with us for a detailed diagnosis and personalised treatment plan.
Frequently asked questions
Yes, cubital tunnel syndrome can cause pain, particularly on the inner side of the elbow. Many individuals experience a dull ache, sharp pain or burning sensation that may extend down to the forearm, and into the hand. Occasionally, the discomfort worsens with prolonged elbow bending, such as when using a phone or driving.
Delaying treatment for cubital tunnel syndrome can lead to progressive nerve damage, resulting in persistent numbness, muscle weakness, and even muscle atrophy in the hand. Additionally, severe cases may cause difficulty in gripping objects or performing fine motor tasks, making everyday activities challenging.
Mild cases of cubital tunnel syndrome may improve with rest, activity modification, and ergonomic adjustments. However, if symptoms persist or worsen, medical treatment may be required to prevent further nerve compression, and long-term dysfunction.
While not all cases of cubital tunnel syndrome are preventable, you can reduce the risk by:
Avoiding prolonged elbow bending.
Maintaining good posture to minimise nerve compression.
Performing gentle stretching, and strengthening exercises to support nerve mobility.
Using elbow padding to protect against excessive pressure.
Recovery time depends on the severity of the condition, and the chosen treatment approach.
Mild to moderate cases often improve within a few weeks to months with conservative treatments like rest, splinting, and physical therapy.
Severe cases requiring surgery may take several months for full recovery, with improvements seen gradually over time.
Some of the noticeable signs that your treatment is effective include:
Decreased discomfort with daily activities like typing, holding a phone, or sleeping.
Improved grip strength, and hand coordination.
Less numbness, and better sensation in the affected fingers.
Reduced pain, and tingling in the elbow, forearm, and fingers.
Yes, cubital tunnel syndrome can recur, especially if underlying risk factors, such as repetitive elbow bending or prolonged pressure on the ulnar nerve, are not addressed. To minimise recurrence, it is important to follow preventive measures, including ergonomic adjustments, strengthening exercises, and proper posture.
At Cove Orthopaedic Clinic, our utmost importance is in helping our patients maintain or regain the mobility that they deserve, all through excellent patient care right from the start.
Happy and satisfied patients are what keeps us going!
Consult Us Today
If you have further enquiries or would like to make an appointment at Cove Orthopaedic Clinic, simply fill in the form below or call us at +65 9631 7637.